
Administrative bulletin: 2026-05-005 Reminders
Date: May 1, 2026
Topics covered in this administrative bulletin are applicable to:
Professional and facility Providers
- Provider data attestation and demographic updates.
- Medically Unlikely Edits (MUE) – Claims editing system update and billing reminder.
- Preventive breast cancer screenings.
Professional Providers only
- CAQH attestation – Reminder.
- Hemophilia clotting factor billing requirements and unit reporting: Claims editing system updates.
- New graduates requesting to join the network.
Facility Providers only
Unless otherwise noted, if you have any questions regarding the information in this bulletin, please contact your Provider Engagement Consultant or visit capbluecross.com/wps/portal/cap/provider/pec-look-up and enter your NPI or Tax ID to identify your designated point of contact at Capital Blue Cross.
Professional and facility Providers
Provider data attestation and demographic updates
- CHIP
- EPO
- FEP PPO
- HMO
- Medicare Advantage HMO
- POS
- PPO
- Traditional and Comprehensive
- Medicare Advantage PPO
KEY POINT: Provider demographic changes must be submitted using the Capital Blue Cross Provider Maintenance and Facility Maintenance tools in our provider web portal, and NOT through Availity’s Provider Data Management tool. Providers are also reminded to review and attest to their data once every 90 days.
Attestation process:
The Provider Maintenance Tool will display the due date and allow providers to review all data that is required in accordance with the Consolidated Appropriations Act, 2021. Once the data has been reviewed, you have two options:
- Attest that the data is accurate.
- No further action is required.
- Attest but updates are required.
- Provider has 3 business days to log back in and update information.
Attestation must be completed as outlined; otherwise, the system will not allow providers to move forward with other day-to-day activities or updates on the tool.
Large groups or health systems should continue using the roster process currently in place directly with Capital.
Demographic change process:
Important Note: On the Availity Essentials home page, you may see a dropdown for Availity’s Provider Data Management Tool. Changes entered into this tool ARE NOT submitted to Capital Blue Cross. Instead, please follow instructions below to ensure you are on the Capital Blue Cross Payer Spaces page.
- Log into Availity. From the home page, select Capital from the Payer Spaces dropdown.
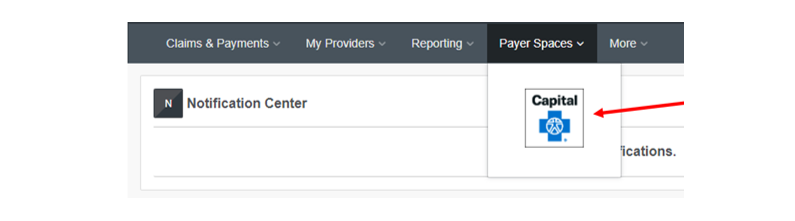
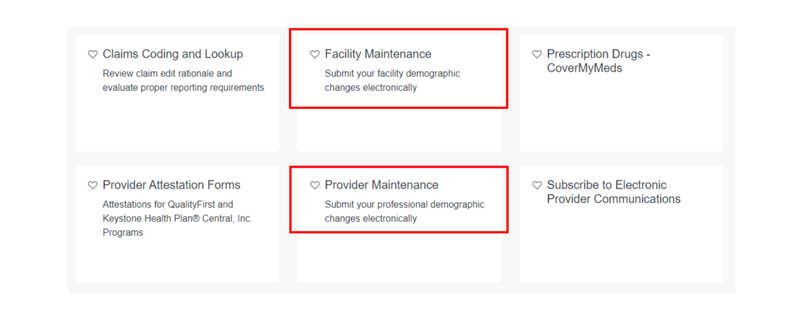
- Click on the Applications tab.
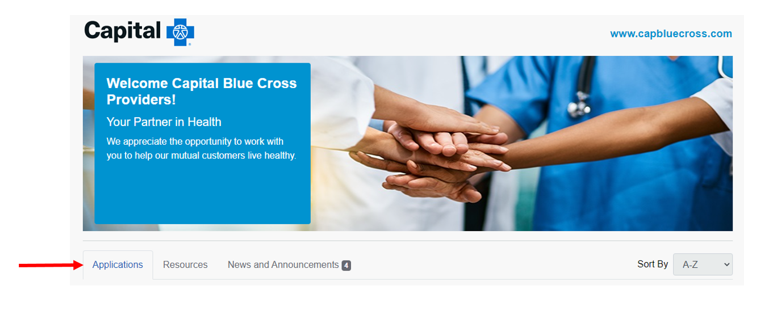
- From here, choose Provider Maintenance to submit your Professional demographic changes electronically, or choose Facility Maintenance to submit your Facility demographic changes electronically.
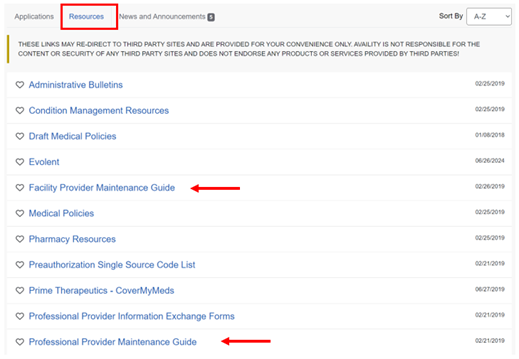
Helpful Guides to completing demographic updates can be found on the Resources tab.
Note to Medicare Advantage Par Providers: Per 42 CFR § 422.111(b)(3), the Centers for Medicare & Medicaid Services (CMS) require Medicare Advantage Organizations to have accurate provider directories, allowing Medicare beneficiaries the ability to identify and locate providers. Therefore, CMS encourages all providers to keep their National Provider Identifier (NPI) data current with the National Plan and Provider Enumeration System (NPPES).
Medically Unlikely Edits (MUE) – Claims editing system update and billing reminder
- CHIP
- EPO
- FEP PPO
- HMO
- Medicare Advantage HMO
- POS
- PPO
- Traditional and Comprehensive
- Medicare Advantage PPO
KEY POINT: Capital is implementing system updates to ensure MUEs are applied consistently and accurately across all provider types. These enhancements correct identified gaps and align our process as communicated in earlier administrative bulletins*.
An MUE for a HCPCS / CPT code is the maximum units of service that a provider would report under most circumstances for a single beneficiary on a single date of service.
There are three (3) types of MUE Adjudication Indicators (MAI)
- MAI 1 – MUE limit applied at the claim line level. Appropriate use of modifiers will enable reporting of medically necessary units of service greater than the MUE limit.
- MAI 2 – MUE limit applied based on date of service. CMS has not identified any instances where a higher value is payable.
- MAI 3 – MUE limit applied based on date of service. In rare or unusual circumstances, additional units may be considered for reimbursement. These MUE denials may be appealed with supporting documentation.
MUE limits applied at the claim line level (MAI 1)
When units of service exceed the MUE value, report as follows:
- Units reported on each line must not surpass the limit.
- When billing multiple lines for the same service, append modifiers such as 76, 77, 91, RT, or LT as appropriate.
Claim lines with units that exceed the MUE value are not eligible for payment.
Correct |
Incorrect |
|---|---|
|
Line 1 – Procedure J7214, 7500 units. (Line MUE is 7500) Line 2 – Procedure J7214, 756 units. (Excess units will be eligible for payment) |
Line 1 – Procedure J7214, 8256 units. (Will deny all units) |
MUE limits applied based on date of service (MAI 2 or 3)
When reporting units of service for the same date that exceed the MUE value, report as follows:
- Report units up to the MUE on one line.
- Report units over the MUE value on the subsequent line.
This allows the units of service up to the MUE value to be eligible for payment.
Correct |
Incorrect |
|---|---|
|
Line 1 – Procedure J1568, 300 units. (MUE is 300) Line 2 – Procedure J1568, 20 units. (Excess units will deny) |
Line 1 – Procedure J1568, 320 units. (Will deny all units) |
References:
FP 01.001 Correct Coding and Reimbursement Methodology
Administrative Bulletin: 2022-06-001
Administrative Bulletin: 2022-12-001
Administrative Bulletin: 2025-05-002
Preventive breast cancer screenings
- CHIP
- EPO
- FEP PPO
- HMO
- Medicare Advantage HMO
- POS
- PPO
- Traditional and Comprehensive
- Medicare Advantage PPO
KEY POINT: This bulletin provides guidance on additional imaging covered as preventive when it is recommended to complete the preventive breast cancer screening process or to address findings identified on the initial preventive screening mammogram.
In alignment with state and federal mandates, Capital Blue Cross’ preventive coverage includes mammographic examinations for covered persons age 40 and older (and for those under 40 when recommended by the member’s physician).
For women at average risk of breast cancer, preventive coverage also includes additional imaging—such as mammography, MRI, and ultrasound—and, as of January 1, 2026, pathology evaluation (biopsy) when it is recommended to complete the preventive screening process or to address findings identified on the initial preventive screening mammogram.
Providers should ensure that all additional screening services and any pathology evaluation performed as part of the initial preventive breast cancer screening to determine malignancy are billed as preventive until a diagnosis is established.
Additionally, as of January 1, 2026, for both breast and cervical cancer screenings, coverage will include patient navigation services and follow-up, when applicable, to support adherence to screening recommendations based on the patient’s assessed need for navigation support.
Providers are encouraged to review the Preventive Services Health Coverage Guidelines, available under “Education and Manuals” in the Provider Library on our provider web portal, to ensure members receive eligible preventive services with no cost-share when applicable.
Additional resource guidance:
Patient Navigation Services for Breast and Cervical Cancer Screening Recommendations | WPSI
Professional Providers only
CAQH attestation – Reminder
- CHIP
- EPO
- FEP PPO
- HMO
- Medicare Advantage HMO
- POS
- PPO
- Traditional and Comprehensive
- Medicare Advantage PPO
KEY POINT: Providers must ensure their Council for Affordable Quality Healthcare (CAQH) application is updated at least every 120 days.
Providers can remain compliant by:
- Reviewing your CAQH application regularly.
- Ensuring all information is up to date and accurate.
- Completing the re-attestation process every 120 calendar days.
Failure to re-attest within the 120-day timeframe may result in delays in credentialing, contracting, and/or network participation.
More information is available by visiting CAQH For Providers or by calling 888.600.9802. Your cooperation in adhering to this requirement is greatly appreciated.
Hemophilia clotting factor billing requirements and unit reporting: Claims editing system updates
- CHIP
- EPO
- FEP PPO
- HMO
- Medicare Advantage HMO
- POS
- PPO
- Traditional and Comprehensive
- Medicare Advantage PPO
KEY POINT: Effective June 1, 2026, Capital will be enhancing our claims editing system to better support the application of correct coding guidelines for Hemophilia factor products.
Providers are reminded to ensure the quantity billed (QB) accurately reflects the number of international units (IU), milligrams (mg), or micrograms (mcg) administered, as defined in the HCPCS code descriptor.
Following conversion of the administered dosage into billable units, claims must be assessed to ensure compliance with correct coding guidelines. Multiple claim lines are required when:
- The units of service exceed the line level MUE limit (MAI 1) assigned to that HCPCS code, or
- The units exceed the system maximum of 9,999 units per claim line.
For the same HCPCS code and the same date of service, no single claim line may exceed either the MUE limit or the 9,999 unit system limit maximum. If total units exceed either limit, the units must be divided and billed across multiple claim lines, following all applicable modifier and coding rules.
MUE limits applied at the claim line level (MAI 1)
When units of service exceed the MUE value, report as follows:
- Units reported on each line must not surpass the limit.
- When billing multiple lines for the same service, append modifiers such as 76, 77, 91, RT, or LT as appropriate.
Claim lines with units that exceed the MUE value are not eligible for payment.
Example:
J7214 (Injection, Factor VIII/von Willebrand factor complex) has an MUE of 7500 units per claim line.
Correct |
Incorrect |
|---|---|
|
Line 1 – Procedure J7214, 7500 units. (Line MUE is 7500) Line 2 – Procedure J7214, 756 units. (Excess units will be eligible for payment) |
Line 1 – Procedure J7214, 8256 units. (Will deny all units) |
For details on FP 01.001 – Correct Coding and Reimbursement Methodology, refer to Capital’s Reimbursement Policies.
Additional information is available via the CMS Practitioner Services MUE Table.
New graduates requesting to join the network
- CHIP
- EPO
- FEP PPO
- HMO
- Medicare Advantage HMO
- POS
- PPO
- Traditional and Comprehensive
- Medicare Advantage PPO
KEY POINT: Requirements for new graduates requesting to join the Capital Blue Cross network.
All new graduates must have completed all their post-graduate education prior to submitting their request to join the network. In addition, providers must also have been granted admitting privileges with at least one participating hospital that is designated as their primary admitting facility (for physicians that admit patients) or have other arrangements for hospitalization that have been approved by Capital Blue Cross prior to submitting their request to join the network.
Physicians who are not required to have admitting hospital privileges are anesthesiologists, allergists, emergency room physicians, dermatologists, pathologists, and radiologists.
Facility Providers only
Urgent and emergent admission notification
- CHIP
- EPO
- FEP PPO
- HMO
- Medicare Advantage HMO
- POS
- PPO
- Traditional and Comprehensive
- Medicare Advantage PPO
KEY POINT: Providers are reminded to notify Capital Blue Cross within appropriate timeframes for urgent and/or emergent inpatient admissions.
Urgent and/or emergent inpatient admissions require notification to Capital within 2 business days from admission. Failure to notify Capital may result in denial.
More information can be found in the Capital Blue Cross Provider Manual, Chapter 5, Unit 1 – Concurrent Review.